Patellar luxation, most often medial patellar luxation (MPL), is a common condition in dogs. The diagnosis and treatment decision-making process are often straight-forward.
If a dog has a frequent skipping lameness then surgical correction is likely to be advised. For most dogs this will mean a tibial crest transposition combined with a femoral trochlear sulcoplasty and a lateral parapatellar imbrication.
Grade I cases of patellar luxation
There are a couple of scenarios however where the decision making is a little more complex. The first of these is the dog diagnosed with an incidental patellar luxation -i.e. one that is not causing clinical signs of lameness or skipping. I do not mean the incidental grade I cases here -grade I meaning that the patella can be manually luxated but it reduces spontaneously and immediately and it is stable at all other times. Grade I cases are invariably of no clinical consequence and surgery is not indicated.
Grade II cases of patellar luxation
But what about the grade II case with no clinical signs? Grade II means that the patella is intermittently and spontaneously luxating during movement. Grade II MPL often presents as a skipping lameness but in some dogs it can be clinically silent. It is possible to make a good argument for and against surgical stabilisation in these patellar luxation cases, and different surgeons will have different view-points on this.
The argument for surgery is that:
- Over time the cartilage on the underside of the patella will wear away from repeated luxation.
- Surgery is therefore considered protective against femeropatellar osteoarthritis (OA).
The argument against surgery is that:
- Not every dog will develop clinically significant OA.
- Therefore, some dogs will be operated on unnecessarily.
In one small study half of non-symptomatic dogs with grade II MPL developed chronic lameness or required surgery (4 years follow-up). Furthermore, a badly performed sulcoplasty may itself damage the patella cartilage and cause OA.
So, how do I approach these cases? As always, it’s important to consider each patient individually. I will consider biomechanical factors; not all grade II cases are the same -some patellas are more unstable than others. Other patient considerations include:
- Age of dog
- Size of dog
- Level of dog’s activity
- Status of the contralateral patella
I’m very likely to recommend surgery in a young, active dog having surgery on the opposite side. The two surgeries can be performed at the same time meaning reduced cost for the owner and only one period of convalescence for the dog. An older, less active dog is more likely to be managed conservatively.
Grade III and IV cases of patellar luxation
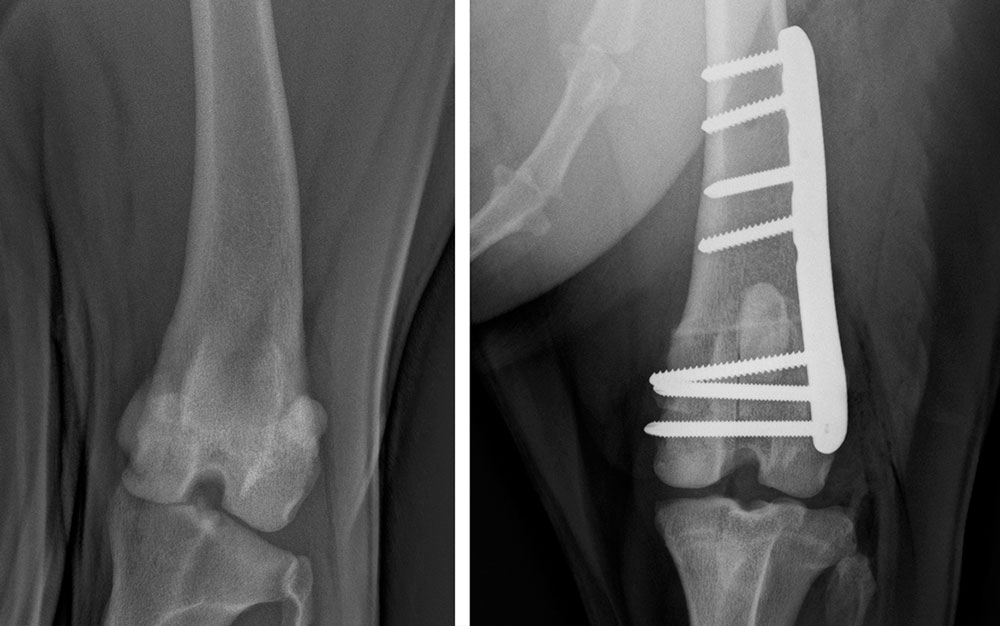
The second scenario where decision making may not be straight-forward is the dog with a more severe grade of MPL -i.e. grade III (the patella is permanently luxated but can be reduced) or grade IV (permanently luxated and can’t be reduced). These dogs generally have a complex combination of femoral and tibial deformities and the dilemma here is not whether to perform surgery or not, but what type of surgery to perform.
Broadly speaking the choice is whether to perform a ‘traditional’ correction (i.e. tibial crest transposition, sulcoplasty, etc) or whether to also address the underlying deformity. For the latter, the most common scenario is a corrective osteotomy of the distal femur to address a distal femoral varus deformity. In some cases femoral and tibial osteotomies may be combined.
Surgical choices
A corrective osteotomy is more complex to plan and perform. It will require more expensive implants than a traditional surgery, with obvious cost implications for the owner. Often the first step in managing these cases therefore is to have a considerate conversation with the owner regarding finances. If I am suspicious of an underlying angular deformity, then I will want to assess this with a CT scan. However, if finances preclude the more complex surgery then the CT scan becomes irrelevant and this additional expense can be avoided for the owner. When we do CT these cases we find a range of distal femoral varus angles. A small amount of distal femoral varus is normal and there are no specific rules for what constitutes a degree of varus which must be corrected. Surgical recommendations are made based on the degree of the deformity, the severity of the MPL and of course individual patient factors.
Needless to say, there is some subjectivity to this process and it is important that your surgeon has the experience and expertise to advise appropriately.

Andy Moores is one of the most qualified and experienced small animal orthopaedic surgeons in the UK. He has been a referral-only orthopaedic surgeon for over 20 years, an EBVS Specialist for 17 years and an RCVS Specialist for 16 years. He has treated thousands of cats and dogs with orthopaedic problems during this time. This experience will be available to your clients and patients at The Moores Orthopaedic Clinic from May 2023. If you would like to discuss a case or make a referral then you can contact Andy directly via andy@mooresortho.com. You can subscribe to our newsletter and be informed of future blogs and articles at www.mooresortho.com